Living Longer, Living Better Navigating, Leveraging and Measuring the Pathways to Longevity
Proposal architect & originating authorMarschall S. Runge, M.D., Ph.D.Executive Vice President for Medical Affairs · CEO Michigan Medicine · Dean UMMS
Proposed PI roster (per doc 1, §"Specific Aims"):Steven L. Kunkel, Ph.D. (PI) ·
Brian D. Athey, Ph.D. (co-PI) ·
Sachin Kheterpal · Scott W. Ballinger · Ryan E. Mills · Greg Farnum
aging-genomicsmitochondria + inflammagingcardiorespiratory fitnessBioButton real-timeCRISPR Perturb-seqOracle Health · Ellison
Aging-genomics is the natural extension of pharmacogenomics. Where pharmacogenomics asks
which drug is right for which person, given their genome?, aging-genomics asks
which way of living and which interventions are right for which person, given their genome,
epigenome, mitochondrial state, and real-time physiology?
Measure → Model → Intervene → Re-measure — at the scale of Oracle Health (150 M EHR via Ellison Institute).
This proposal grounds longevity research in rigorously-validated biomarkers and longitudinal data — not the silver-bullet rhetoric of the longevity-influencer marketplace.
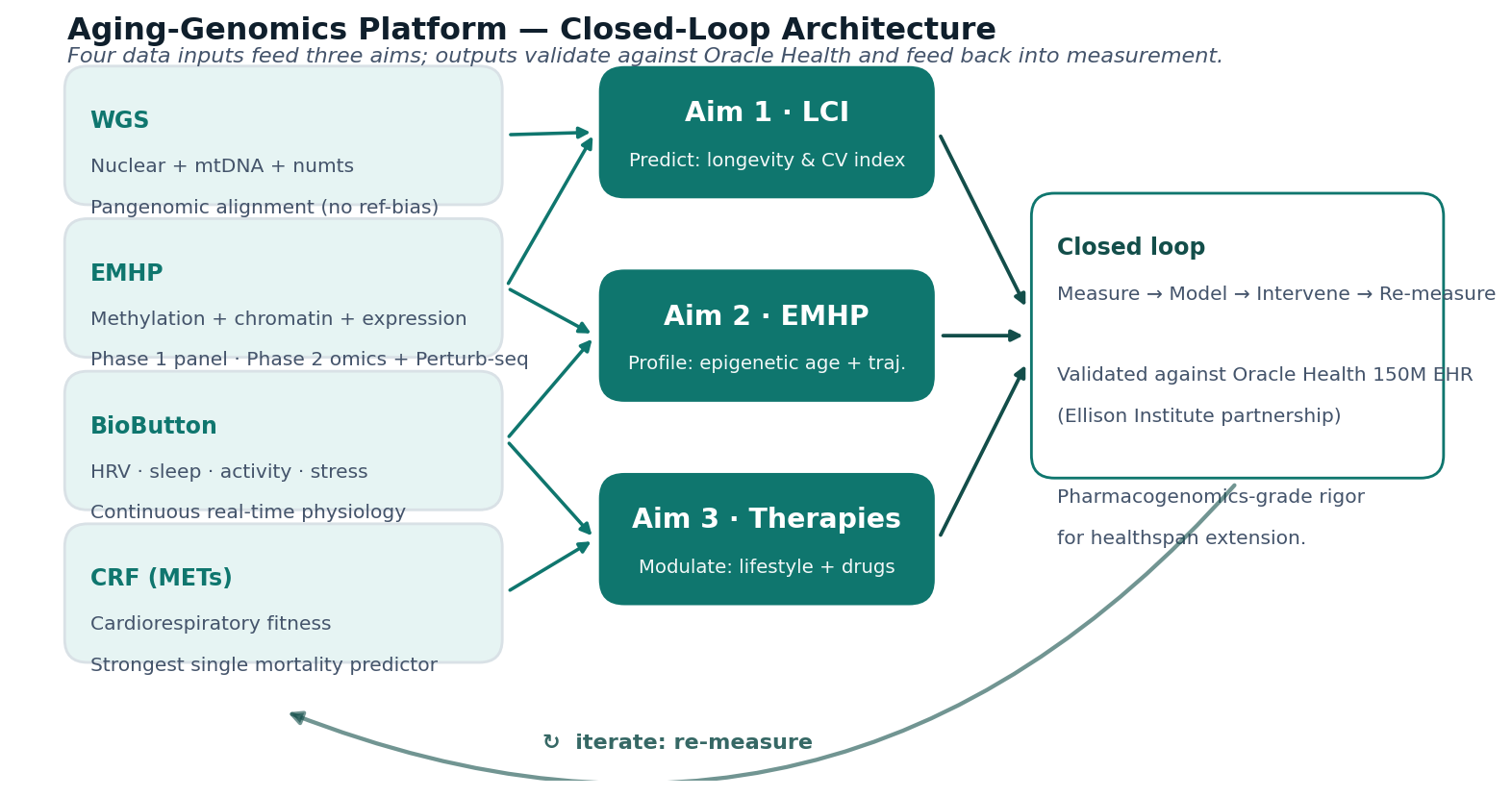
Three aims deliver a closed-loop measure → model → intervene → re-measure system at the scale of Oracle Health.
Read these first
Three doors into the proposal, ranked by how fast you can be on the same page as the team:
Closed-loop precision longevity: measure → model → intervene → re-measure, with the rigor pharmacogenomics has brought to oncology and cardiology.
Aim 1 · Measure
LCI — Longevity & Cardiovascular Health Index
A clinically-deployable predictive index integrating nuclear and mitochondrial WGS, cardiorespiratory fitness (METs from exercise stress testing), standard clinical risk factors, and continuous BioIntelliSense BioButton physiology (HRV, sleep architecture, activity, stress signatures).
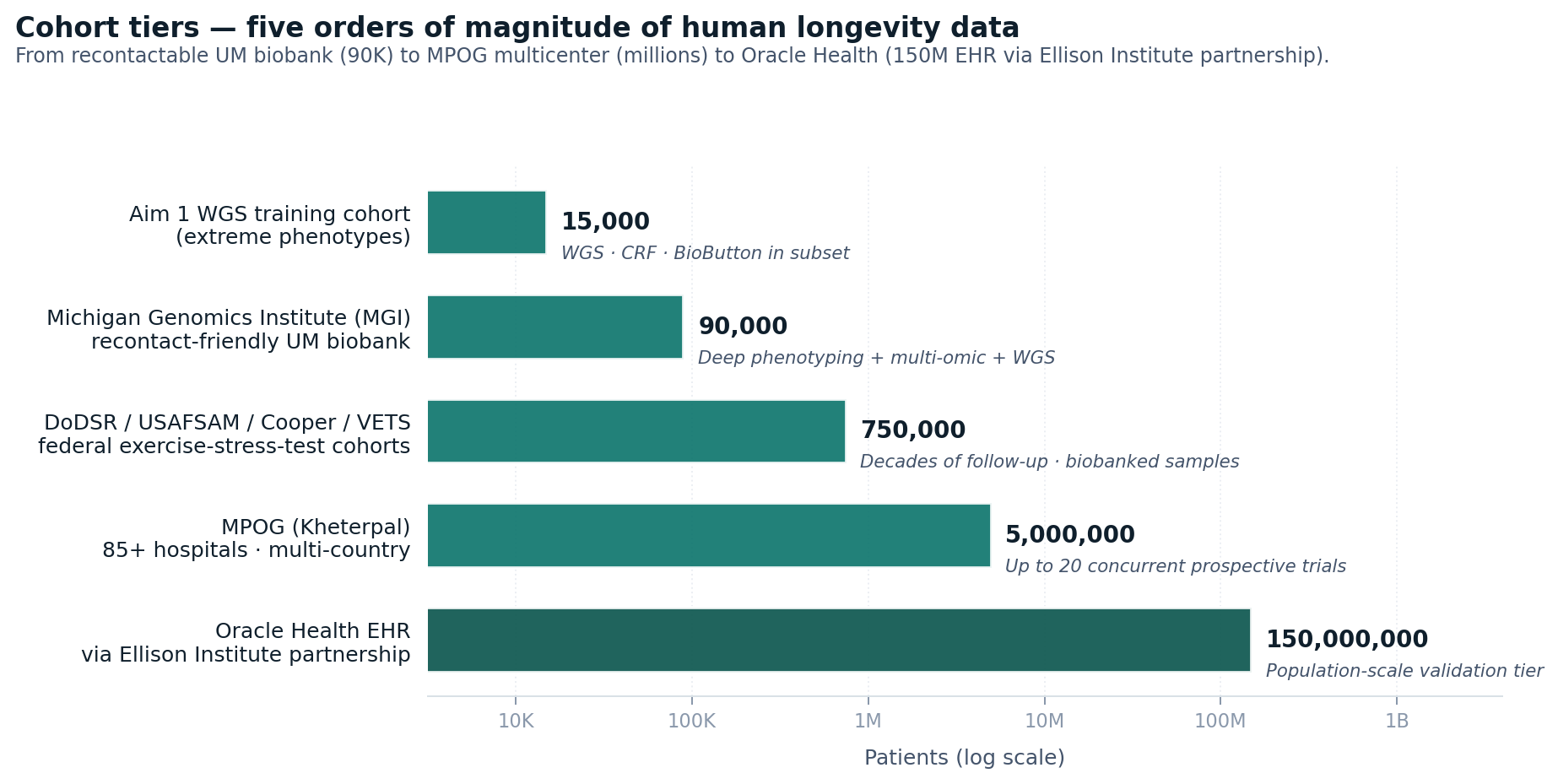
Cohorts: MGI (~90K UM patients) · MPOG (Kheterpal, millions of records, 85+ hospitals) · DoDSR / USAFSAM / Cooper / VETS (federal exercise-stress-test cohorts) · Oracle Health 150M EHR (Ellison Institute partnership).
Outcome: Patented Ellison-branded diagnostic algorithm embedded in Oracle Health clinical decision-support, population-health, and employer/payer products.
Phase 2: genome-wide methylation (EPIC arrays, RRBS/WGBS), chromatin profiling (ATAC-seq, ChIP-seq), and CRISPR Perturb-seq in patient-derived iPSCs for causal-flow discovery — distinguishing biomarkers from actionable therapeutic targets.
Outcome: CLIA/IVD blood-based panel with OCI-hosted interpretive software outputting epigenetic age, biological-age trajectory, and intervention response.
Aim 3 · Intervene
Targets, Therapies & Precision Longevity Programs
Network analysis prioritizes epigenetic enzymes (DNMTs, TETs, HDACs, sirtuins) and mitochondrial regulators for therapeutic modulation. Drug discovery uses EMHP + LCI as pharmacodynamic readouts and BioButton as continuous responder-monitor.
The aging-genomics decision framework (architected by Athey, pharmacogenomics-analogous) integrates genotype + epigenotype + LCI + BioButton phenotypes to output individualized lifestyle prioritization (sleep / movement / stress / diet / social-purpose) and therapeutic-candidate identification.
Integration: Oracle Health clinical workflows, EIT-affiliated longevity clinics, employer/payer offerings.
Mechanistic core
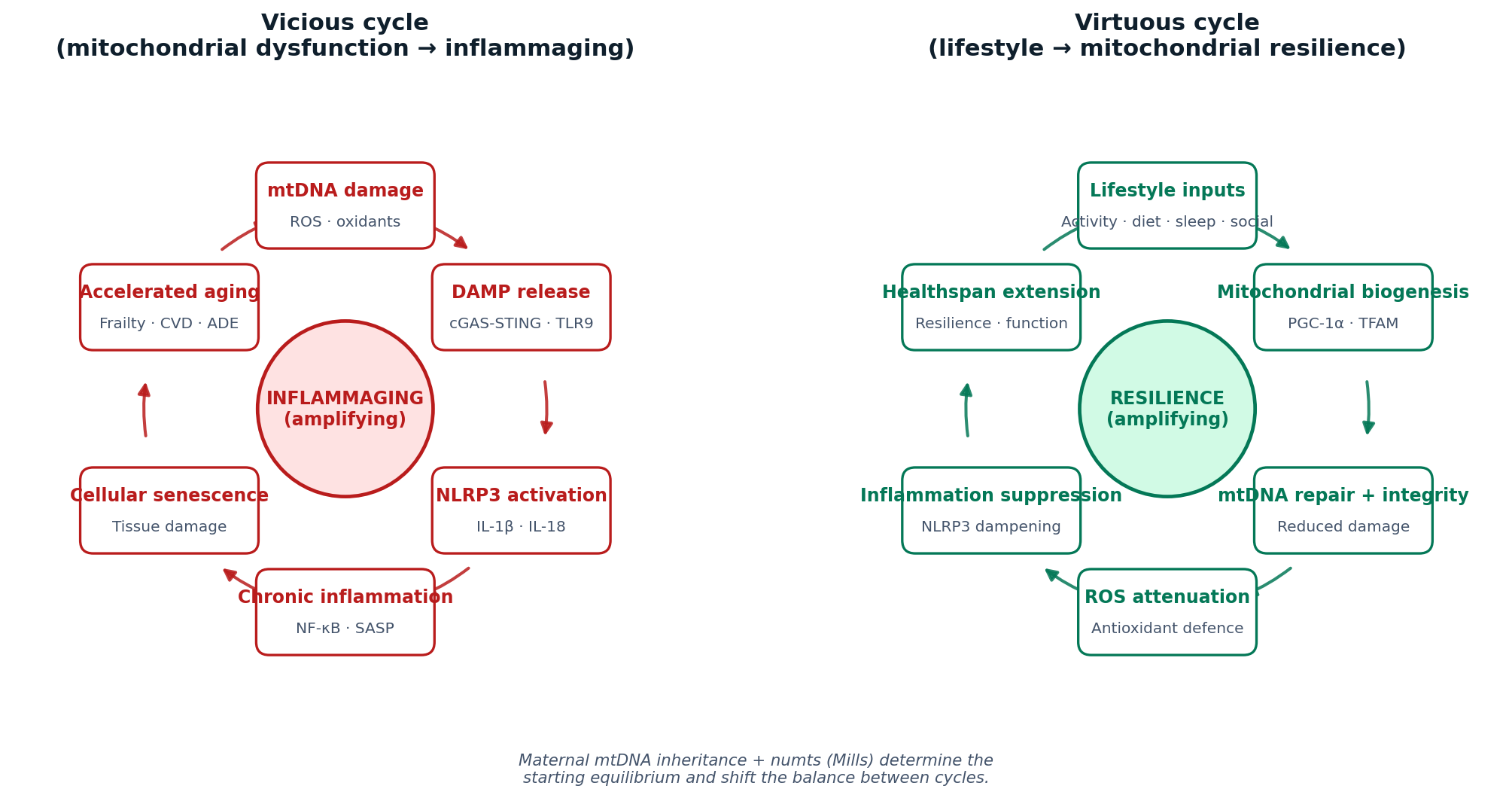
Mitochondrial-inflammaging axis: dysfunctional mitochondria release mtDNA-DAMPs and reactive oxygen species, activating the NLRP3 inflammasome / NF-κB and chronic inflammation that accelerates aging. Lifestyle modulates this axis through epigenetic regulation. Maternal mtDNA inheritance + numts (Mills's numtogenesis methodology) layer a largely-overlooked genetic dimension on top of the canonical Ballinger-Runge mtDNA-atherosclerosis story.
At a glance — eight figures
The platform's mechanisms, study design, and program timeline rendered as auto-generated figures (matplotlib; PDF + PNG live in figures/ and rebuild on every push).
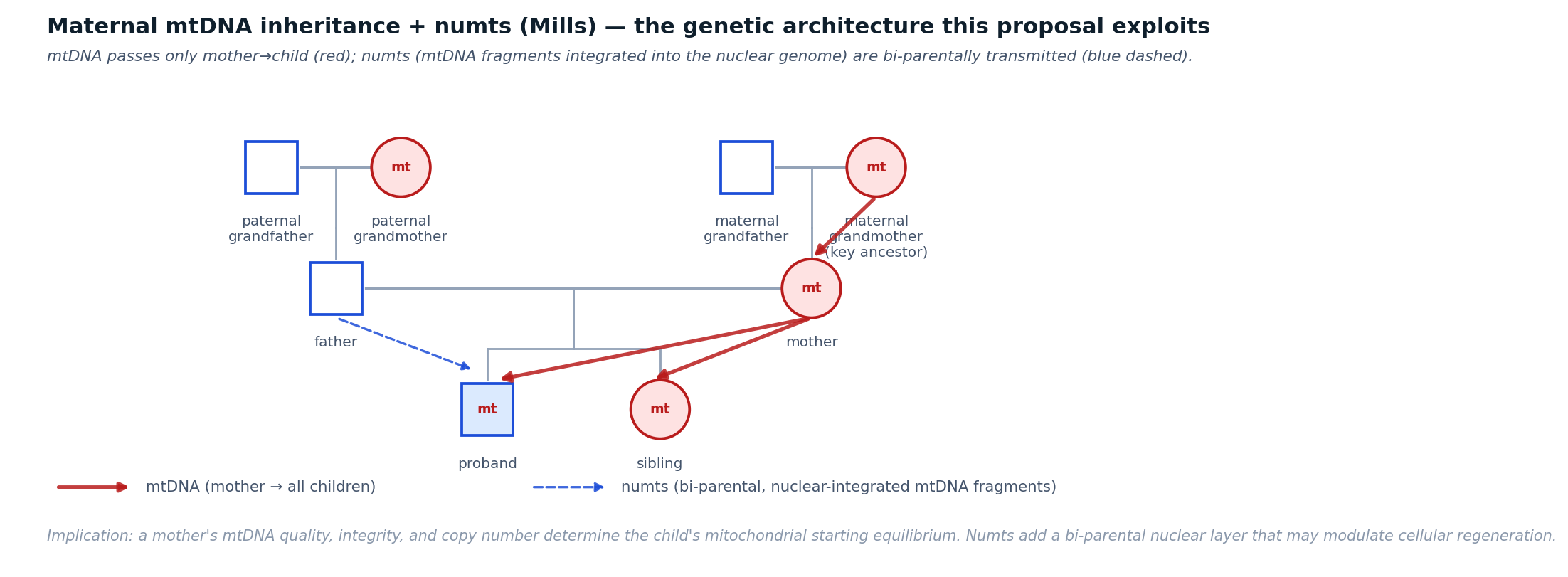
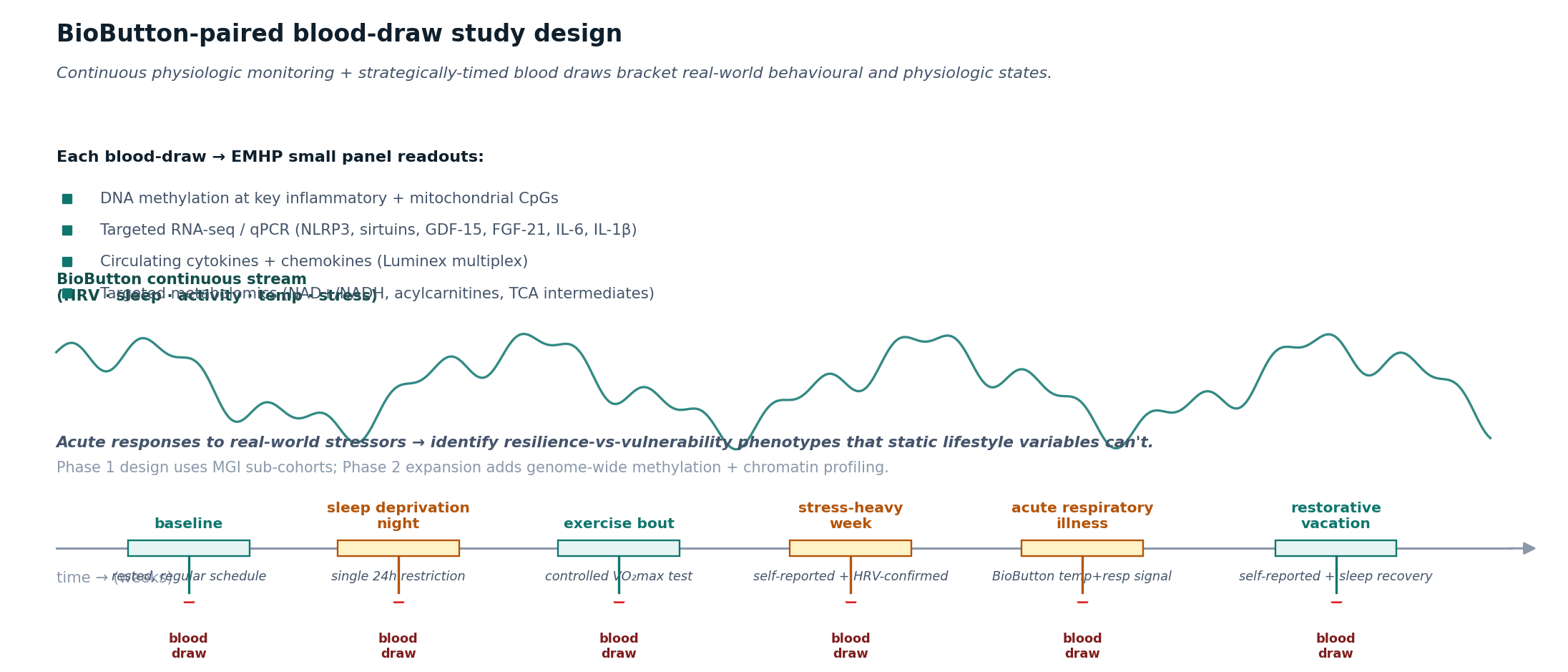
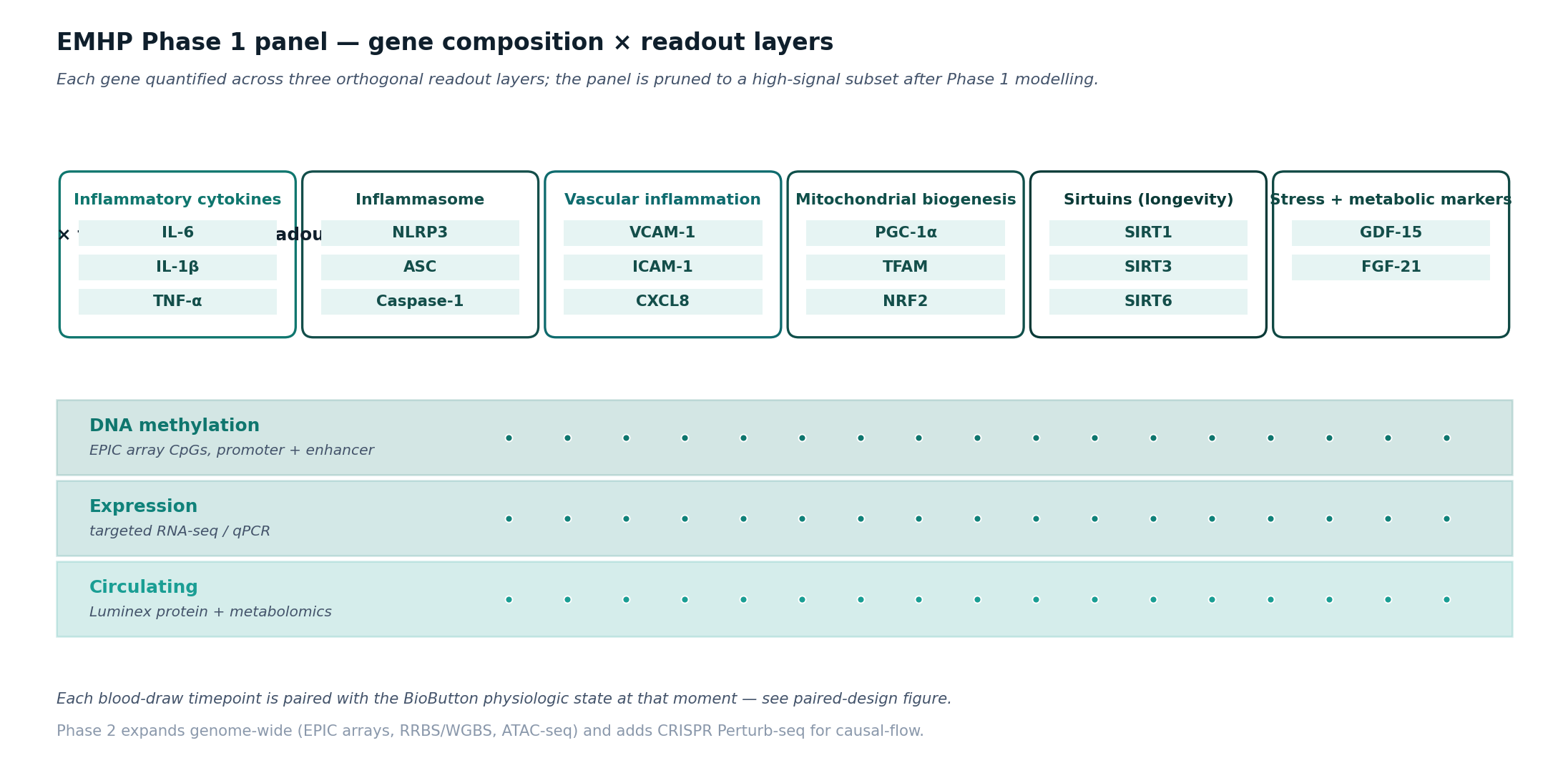
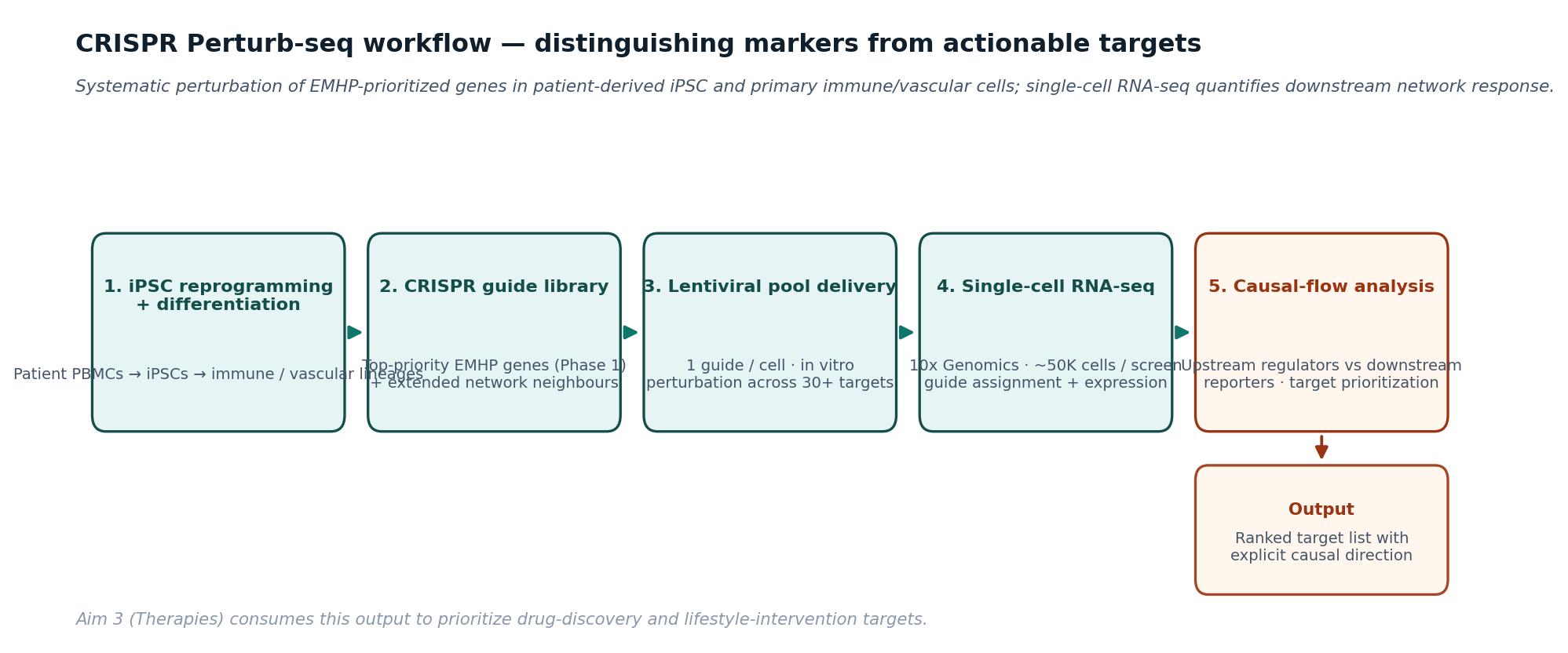
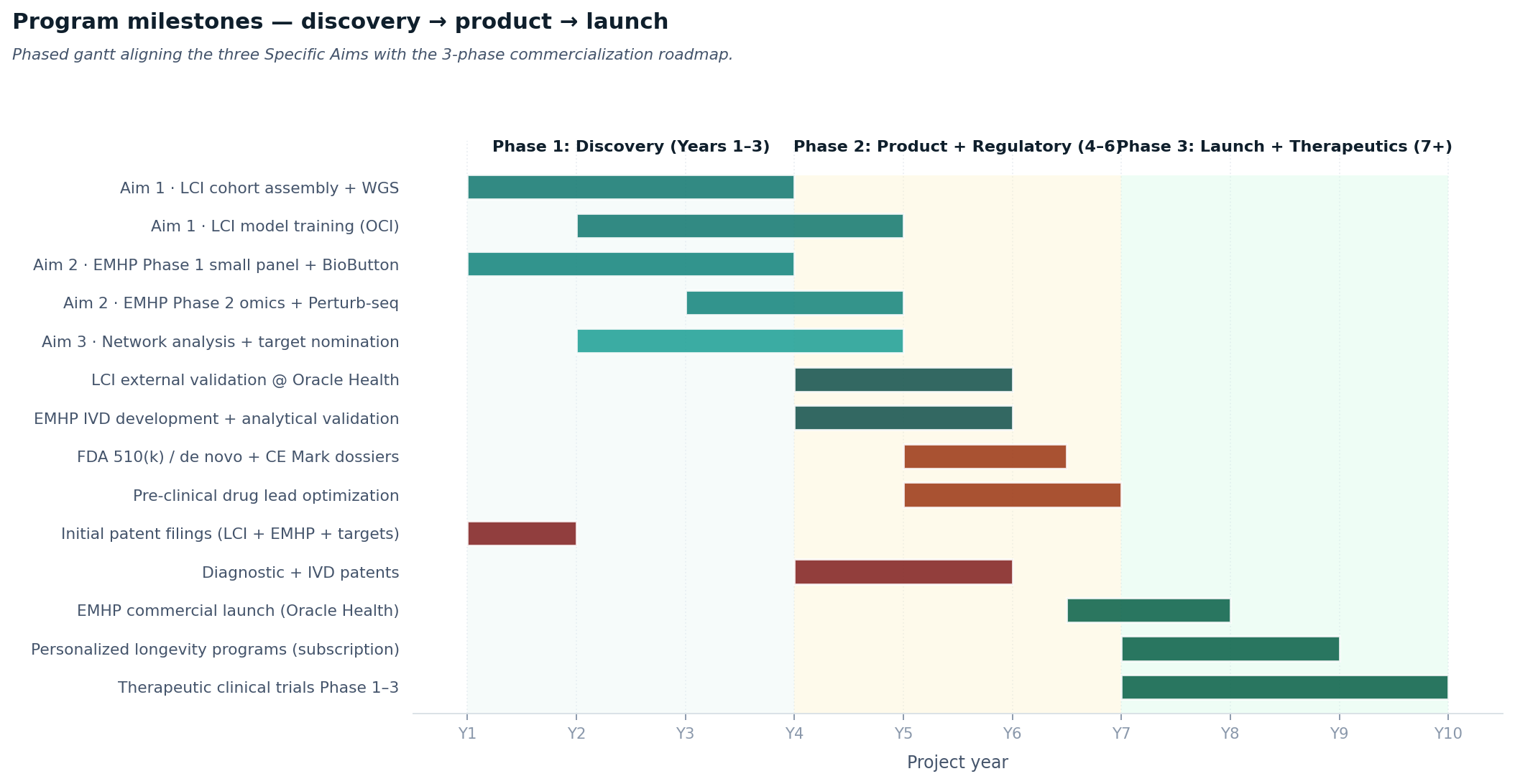
Figure 1. Aging-genomics closed-loop architecture. Four data inputs (WGS, EMHP, BioButton, cardiorespiratory fitness) feed three aims; outputs validate against the Oracle Health 150M EHR via the Ellison Institute partnership and feed back into iterative measurement.Figure 2. Five orders of magnitude of human longevity data, anchored at the WGS-rich Aim 1 training cohort and validated at population scale through Oracle Health.Figure 3. The mechanistic spine. Left: dysfunctional mitochondria release mtDNA-DAMPs and ROS, activating NLRP3 / NF-κB and chronic inflammation that drives senescence, tissue damage, and accelerated aging. Right: lifestyle inputs (activity, diet, sleep, social) drive mitochondrial biogenesis, mtDNA repair, ROS attenuation, and inflammation suppression — the virtuous cycle of healthspan extension. Maternal mtDNA inheritance + numts (Mills) determine the starting equilibrium.Figure 4. Maternal mtDNA inheritance + numts. mtDNA is transmitted exclusively through the maternal line (red); numts (mtDNA fragments integrated into the nuclear genome, characterized methodologically by Mills) are bi-parentally inherited (blue dashed). The mother's mitochondrial template determines the offspring's mitochondrial starting equilibrium; numts add a nuclear layer that may modulate cellular regeneration.Figure 5. The BioButton-paired-blood-draw design (Aim 2 Phase 1). Continuous BioIntelliSense BioButton physiologic data (HRV, sleep, activity, temperature, stress) above the timeline; strategically-timed blood draws below capture EMHP small-panel readouts (methylation, expression, circulating proteins, metabolites) at defined behavioral and physiologic states. Acute responses to real-world stressors identify resilience-vs-vulnerability phenotypes that static lifestyle variables cannot.Figure 6. EMHP Phase 1 panel composition. Each gene is quantified across three orthogonal readout layers — DNA methylation at promoter / enhancer CpGs (EPIC array), expression (targeted RNA-seq / qPCR), and circulating protein or metabolite (Luminex multiplex / metabolomics). The panel is pruned to a high-signal subset after Phase 1 modeling; Phase 2 expands to genome-wide methylation and chromatin profiling.Figure 7. CRISPR Perturb-seq workflow (Aim 2 Phase 2). Patient-derived iPSCs are differentiated to immune / vascular lineages; a focused CRISPR guide library (EMHP-prioritized genes plus extended network neighbors) is delivered by lentiviral pool; single-cell RNA-seq quantifies guide identity and downstream transcriptomic response per cell. Causal-flow analysis distinguishes upstream regulators (actionable therapeutic targets) from downstream reporters (biomarkers only).Figure 8. Program milestone timeline aligning the three Specific Aims with the 3-phase commercialization roadmap. Discovery (Years 1–3) executes the aims and files initial patents; Product (Years 4–6) refines EMHP into a clinical-grade IVD with FDA 510(k) / de novo and CE Mark dossiers, plus pre-clinical drug lead optimization; Launch (Years 7+) deploys EMHP through Oracle Health and longevity-clinic channels, advances therapeutic candidates through clinical trials.
Tables
Four auto-generated reference tables. Full versions on the standalone tables page; LaTeX sources in tables/ for direct inclusion in long-form variants.
28 funding-mechanism PDFs are bundled directly into this site — no GitHub round-trip, click and read. CI rebuilds them all on every push to main. Word counts are current build (long-form variants are intentionally over their nominal page budget; trim at submission time).
Long-form Research Strategy 🔧 trim at submission
The full proposal: 3-aim Research Strategy + Significance + Innovation + Environment + Commercialization roadmap + 8-section NIH-required Appendix + 6 PI biosketches.
Recommended first submission
NIA R01 — aging biomarker
12 pages · ~6,171 words · NIH NIA
Full 12-page R01 framed for NIA program review (aging-biomarker emphasis). The 4-axis aging framing fits NIA more naturally than a generic R01.
Best for: Marschall & Steve choosing the first formal submission.
Standard NIH R01 Research Strategy. Same content as NIA R01 with mechanism-neutral framing — the right fit if NHLBI or NIGMS is the better study-section match for the cardiovascular-translation angle.
Best for: NHLBI / NIGMS / NIDDK study-section reviewers.
NIA U19 Specialized Center format — adds a Project Synopsis section, Multi-PI Leadership Plan, and explicit core/sub-project structure. Best fit for a coordinated 5-PI center submission.
Best for: a coordinated multi-PI center submission (Kunkel + Athey + Kheterpal + Runge + Mills).
Texas Cancer Prevention and Research Institute format. Long-form Research Strategy with cancer/age-related-disease emphasis (cellular senescence, SASP, somatic mosaicism connection to oncogenesis).
Best for: a Texas-based co-investigator or partnership angle.
NSF Project Summary format with explicit Overview + Intellectual Merit (3 methodological advances) + Broader Impacts (5 dimensions: public health relevance, training, diversity-in-research-populations, open science, distinguishing-rigorous-from-hype, commercialization with public-health intent).
Best for: existing NSF awardee adding an aging supplement.
Training-program-focused application (not recycled R01). Project Summary + 4 Specific Aims of the training program (cross-axis recruitment, training environment, K99/R00 pipeline, diversity recruitment) + Research Training Plan + biosketches.
Best for: training pipeline at the inflammation × computational-medicine intersection.
DARPA-BTO Heilmeier Catechism format with operational-resilience framing. Same 9-question structure as ARPA-H, with explicit Year 1 / 3 / 5 / 7 milestones and risk-mitigation enumeration that DARPA program managers expect.
Best for: DARPA solicitation aligned with operational performance and recovery metrics.
Foundation-grant format with explicit theory of change (the field is not technology-limited; it is disciplined-translation-limited), why-this-team (mechanism + infrastructure + translation), per-phase deliverables, and a flexible mechanism-appropriate ask.
Best for: Schmidt Futures longevity / health-platform call.
Open Philanthropy format with the same theory-of-change framing. Anti-influencer-hype framing matches Open Phil's empirical bar; explicit causal logic from funding gap to deployed deliverables.
Best for: Open Philanthropy longevity-research call.
Hand-authored lay-friendly summary (5 sections: what it is in plain language · what we will measure · what we will deliver · why now · why Michigan). Distinct from the technical Project Summary — this one is press-office-ready, with no jargon and no methodology weeds.
Best for: press office, donor briefs, public-facing announcements.
Hand-authored Perspective essay arguing that aging-genomics is the natural extension of pharmacogenomics. Sections: longevity question is no-longer-hypothetical · paradigm extension · what's technically tractable now · what remains hard · platform program structure · why framing matters · acknowledgements.
Best for: establishing the conceptual frame in a high-visibility venue, as companion piece to the funded grant.
2-page concept paper for cold outreach to potential collaborators (additional cohort holders, philanthropic partners, technology companies). Heavy on "aging-genomics extends pharmacogenomics" framing.
Best for: introductory emails to new collaborators.
Single-page non-technical summary for senior leadership, board members, or philanthropic sponsors who need the core idea without the methodology weeds.
Best for: board prep, donor briefs, leadership read-aheads.
EMHP refined to clinical-grade IVD. FDA 510(k) or de novo + CE Mark dossiers. Pre-clinical drug lead optimization with EMHP and LCI as pharmacodynamic readouts and BioButton as continuous responder-monitor.
Phase 3 · Years 7+
Commercial Launch & Therapeutic Translation
EMHP launched via Oracle Health and longevity-clinic channels. Personalized longevity programs licensed to employer/payer wellness programs. Therapeutic candidates advance through Phase 1–3 trials.
Where we are
Quick status across the eleven things that gate a real submission.
3-aim Research Strategy prose
Drafted from Marschall's source documents. Long-form variants build at ~6,200 words; mid-page at ~3,000.
All compile in CI on every push. Direct downloads bundled into this dashboard.
References (refs.bib, 48 entries)
Populated from doc 1's reference list (inflammaging mechanism, mtDNA-atherogenesis foundation, epigenetic clocks, exercise epigenetics, partial reprogramming).
PI biosketches
Drafted from public bibliography (Personal Statement + Positions + Contributions to Science). Each PI replaces with current eRA-Commons-format version at submission.
Human-subjects appendix
Framework drafted (IRB strategy, HIPAA compliance, vulnerable-population coverage). Real IRB protocol architecture pending from Athey.
Multi-PI Leadership Plan
Drafted with cal-mo allocations and conflict-resolution escalation pathway. PIs to confirm allocations at submission time.
Data sharing & resource-sharing plan
Drafted with dbGaP + OCI controlled-access tiers. Specific dataset-by-dataset access governance pending Sachin's MPOG terms and Marschall's Ellison MOU.
Budget justification
Stub only. Real numbers need EVPMA office input (Marschall) and MPOG operational budget (Sachin).
Ellison & Oracle Health partnership terms
Pending Marschall confirmation of EIT MOU and Oracle Health 150M EHR access tier for Aim 1 LCI validation.
MPOG governance terms
Pending Sachin confirmation that MPOG governance supports BioButton-paired-blood-draw sub-cohorts and the EMHP discovery-cohort sampling design.
First submission target
Recommend NIA R01 (aging biomarker emphasis fits NIA program review). Steve and Brian to confirm as PI/co-PI.
Drafted, ready to read Draft in place, PI input needed Blocked on PI decision or external input
What we need from PIs
Pick the first submission target.
NIA R01 (aging biomarker) and the standard R01 are both content-complete. The 4-axis aging framing fits NIA program review better — Steve and Brian, your call as PI/co-PI; Marschall as senior collaborator can advise on Michigan Medicine sponsor letters.
Sign-off pass on Aims and Abstract.
Each PI read the linked Aims page (above) and Abstract (in any long variant) and post comments as
GitHub issues (~30 min each).
Biosketch refresh.
Six PI biosketch atoms are in atoms/prose/biosketches/{kunkel, athey, kheterpal, runge, ballinger, mills}.md.
Each PI replaces with their current eRA-Commons-format biosketch (Personal Statement + Positions + Contributions to Science + Research Support).
Sachin — MPOG governance.
Confirm MPOG governance terms supporting BioButton-paired-blood-draw sub-cohorts and the EMHP discovery-cohort sampling design.
Marschall — Ellison / Oracle Health partnership terms.
Confirm EIT MOU and Oracle Health 150M EHR access tier for Aim 1 LCI validation.
Budget + IRB.budget_justification.md and human_subjects.md are stubs. Need real numbers from the EVPMA office (Marschall) and IRB protocol architecture (Brian).
Source documents (canonical)
Every prose atom, claim, and figure in this proposal traces back to one of these two source documents. If you find anything in the variant PDFs that contradicts these source drafts, the atoms are wrong — fix them, not the sources.
Atom system: prose atoms compose into 26 atom-built variants + 2 hand-authored format-specific (beamer, A0 poster) = 28 PDFs via variants/*.yaml. Every push to main rebuilds all 26 atom-built PDFs in CI and republishes them; this dashboard then bundles them for direct download.